Cranial Cruciate
Ligament Disease
Associated Terms:
Cruciate Disease, Ruptured Cranial Cruciate Ligament, ACL Injury, Torn Cranial Cruciate Ligament, Partial ACL Injury, Tibial Plateau Leveling Osteotomy, Tibial Tuberosity Advancement, Lateral Suture Stabilization, Meniscal Tear
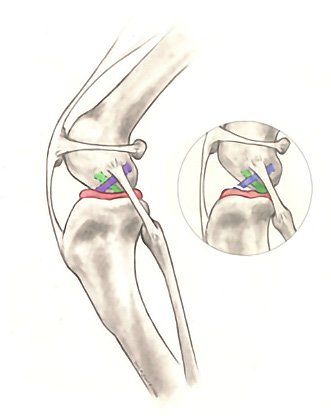
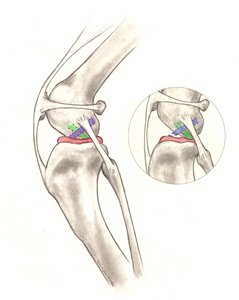 The cranial cruciate ligament (CrCL, see Figure 1.) is one of the most important stabilizers inside the canine knee (stifle) joint, the middle joint in the back leg. In humans the CrCL is called the anterior cruciate ligament (ACL).
The cranial cruciate ligament (CrCL, see Figure 1.) is one of the most important stabilizers inside the canine knee (stifle) joint, the middle joint in the back leg. In humans the CrCL is called the anterior cruciate ligament (ACL).
The meniscus (Figure 1) is a ‘cartilage-like’ structure that sits in between the femur (thigh) and tibia (shin) bones. It serves many important purposes in the joint such as shock absorption, position-sensing, and load-bearing and can be damaged when the CrCL is ruptured.
Rupture of the CrCL is one of the most common reasons for hind limb lameness, pain, and subsequent knee arthritis. Since the development of this problem in dogs is much more complex than in humans, and they experience different degrees of rupture (partial or complete), the canine condition is referred to as ‘cranial cruciate ligament disease’ (CrCLD). While the clinical signs (symptoms) associated with CrCLD vary, the condition invariably causes rear limb dysfunction and pain.
Most commonly CrCLD is caused by a combination of many factors, including aging of the ligament (degeneration), obesity, poor physical condition, genetics, conformation (skeletal shape and configuration), and breed. With CrCLD, ligament rupture is a result of subtle, slow degeneration that has been taking place over a few months or even years rather than the result of acute (sudden) trauma to an otherwise healthy ligament (which is very rare). This difference between people and dogs explains two important features of canine CrCLD:
- 40-60% of dogs that have CrCLD in one knee will, at some future time, develop a similar problem in the other knee.
- Partial tearing of the CrCL is common in dogs and progresses to a full tear over time.
Cranial cruciate ligament disease can affect dogs of all sizes, breeds, and ages, but rarely cats. Certain dog breeds are known to have a higher incidence of CrCLD (Rottweiler, Newfoundland, Staffordshire Terrier, Mastiff, Akita, Saint Bernard, Chesapeake Bay Retriever, and Labrador Retriever) while others are less often affected (Greyhound, Dachshund, Basset Hound, and Old English Sheepdog). A genetic mode of inheritance has been shown for Newfoundlands and Labrador Retrievers.
Poor physical body condition and excessive body weight are risk factors for the development of CrCLD. Both of these factors can be influenced by pet owners. Consistent physical conditioning with regular activity and close monitoring of food intake to maintain a lean body mass is advisable.
Dogs with CrCLD may exhibit any combination of the following signs (symptoms):
- difficulty rising from a sit
- trouble jumping into the car
- decreased activity level
- lameness (limping) of variable severity
- muscle atrophy (decreased muscle mass in the affected leg)
- decreased range of motion of the knee joint
- a popping noise (which may indicate a meniscal tear)
- swelling on the inside of the shin bone (fibrosis or scar tissue)
- pain
- unwillingness to play
- stiffness
Diagnosing complete tears of the CrCL is easily accomplished by a veterinarian using a combination of gait observations, physical examination findings, and radiography (X-rays). By contrast, partial CrCL tears may be more challenging to diagnose.
X-rays allow your veterinarian to:
- confirm the presence of joint effusion (fluid accumulation in the joint, indicating that there is an abnormality present)
- evaluate for the presence/degree of arthritis
- take measurements for surgical planning
- rule out concurrent disease conditions
Specific palpation techniques that veterinarians use to assess the CrCL include the ‘cranial drawer test’ and the ‘tibial compression test.’ These tests can confirm abnormal motion within the knee consistent with rupture of the CrCL.
Many treatment options are available for CrCLD. The first major decision is between surgical treatment and non-surgical (also termed conservative or medical) treatment/management. The best option for your pet depends on many factors including their: activity levels, size, age, skeletal conformation, and degree of knee instability.
Surgical treatment is typically the best treatment for CrCLD since it is the only way to permanently control the instability present in the knee joint. Surgery addresses one of the main issues associated with CrCLD—knee instability and the pain it causes as a consequence of the loss of normal CrCL structural support.
The goal of surgery is not to “repair” the CrCL itself. Due to biological and mechanical influences, the CrCL has no ability to heal once tearing begins regardless of the degree of severity. Unlike in human ACL surgery, the canine CrCL is not typically “replaced” with a graft. This fact is largely due to the major mechanical differences that exist between biped (human) and quadruped (canine) knees that make graft-based techniques less reliable in dogs. If present concurrently, meniscal injury will be addressed by your surgeon by removing the damaged meniscal parts when performing surgery to stabilize the knee. To address knee instability, many surgical treatment options are available. These different techniques can be categorized into two groups based on different surgical concepts:
 Osteotomy-based techniques require a bone cut (osteotomy) which changes the way the quadriceps muscles act on the top of the shin bone (tibial plateau). Stability of the knee joint is achieved without replacing the CrCL itself but rather by changing the biomechanics of the knee joint. This can be accomplished by either advancing the attachment of the muscle (Tibial Tuberosity Advancement (TTA)) or by rotating the plateau (slope) of the shin bone (Tibial Plateau Leveling Osteotomy (TPLO)). Many surgeons prefer these techniques for large, active dogs because of their consistent outcomes in even the most athletic of patients:
Osteotomy-based techniques require a bone cut (osteotomy) which changes the way the quadriceps muscles act on the top of the shin bone (tibial plateau). Stability of the knee joint is achieved without replacing the CrCL itself but rather by changing the biomechanics of the knee joint. This can be accomplished by either advancing the attachment of the muscle (Tibial Tuberosity Advancement (TTA)) or by rotating the plateau (slope) of the shin bone (Tibial Plateau Leveling Osteotomy (TPLO)). Many surgeons prefer these techniques for large, active dogs because of their consistent outcomes in even the most athletic of patients:
- Tibial Plateau Leveling Osteotomy (TPLO) involves making a circular cut around the top of the tibia and rotating its contact surface (tibial plateau) until it attains a near level orientation (approximately 90 degrees) relative to the attachment of the quadriceps muscles (Figure 2). This renders the knee more stable, in the absence of the CrCL. The cut in the bone needs to be stabilized by the use of a bridging bone plate and screws (Figure 3).
; copyright notice: 2012 © Synthes, Inc. or its affiliates. All rights reserved.") Once the bone has healed, the bone plate and screws are not needed, but they are rarely removed unless there is an associated problem (irritation, infection).The perceived advantages of this compared to suture-based techniques are the superior outcomes attained in larger dogs relative to limb function and athletic mobility with less progression of arthritis.The major disadvantage is the need to perform an osteotomy. Any osteotomy requires healing of the bone, and if a problem is observed (such as implant failure, failure of the bone to heal), it may require revision surgery that may negatively affect short and long-term outcomes. Fortunately, such complications are rare, especially when the procedure is performed by an experienced board-certified surgeon.
Once the bone has healed, the bone plate and screws are not needed, but they are rarely removed unless there is an associated problem (irritation, infection).The perceived advantages of this compared to suture-based techniques are the superior outcomes attained in larger dogs relative to limb function and athletic mobility with less progression of arthritis.The major disadvantage is the need to perform an osteotomy. Any osteotomy requires healing of the bone, and if a problem is observed (such as implant failure, failure of the bone to heal), it may require revision surgery that may negatively affect short and long-term outcomes. Fortunately, such complications are rare, especially when the procedure is performed by an experienced board-certified surgeon.  Tibial Tuberosity Advancement (TTA) requires a linear cut along the front of the shin (tibia) bone. The front of the tibia, called the ‘tibial tuberosity’ is advanced forward until the attachment of the quadriceps is oriented approximately 90 degrees to the tibial plateau (Figure 4). This is another way to accomplish the same mechanical advantage offered by the TPLO that renders the knee more stable in the absence of the CrCL. The TTA and TPLO share similar advantages and disadvantages. Similar to the TPLO, the cut in the bone is stabilized by the use of a specifically designed bridging bone plate and screws. The decision between TPLO and TTA is based purely on the opinion of your surgeon and their personal technical experience. To date, no published data supports one technique being superior to the other.
Tibial Tuberosity Advancement (TTA) requires a linear cut along the front of the shin (tibia) bone. The front of the tibia, called the ‘tibial tuberosity’ is advanced forward until the attachment of the quadriceps is oriented approximately 90 degrees to the tibial plateau (Figure 4). This is another way to accomplish the same mechanical advantage offered by the TPLO that renders the knee more stable in the absence of the CrCL. The TTA and TPLO share similar advantages and disadvantages. Similar to the TPLO, the cut in the bone is stabilized by the use of a specifically designed bridging bone plate and screws. The decision between TPLO and TTA is based purely on the opinion of your surgeon and their personal technical experience. To date, no published data supports one technique being superior to the other.
- Tibial Plateau Leveling Osteotomy (TPLO) involves making a circular cut around the top of the tibia and rotating its contact surface (tibial plateau) until it attains a near level orientation (approximately 90 degrees) relative to the attachment of the quadriceps muscles (Figure 2). This renders the knee more stable, in the absence of the CrCL. The cut in the bone needs to be stabilized by the use of a bridging bone plate and screws (Figure 3).
- Suture-based techniques can be divided into intra-articular (within the joint) and extra-articular (outside the joint) procedures. Because of the inconsistency of the results reported with intra-articular techniques in dogs, suture-based procedures are primarily performed in an extra-articular fashion. The most commonly performed technique is called extra-capsular suture stabilization, which utilizes suture material that is placed just on the outside of the knee joint (but under the skin) to mimic the stability offered by the CrCL. A variation of this technique is called Tightrope® and allows the surgeons to use bone tunnels for proper suture placement.
- Extra-capsular suture stabilization (also called “Ex-Cap suture,” “lateral fabellar suture stabilization,” and the “fishing line technique”) is a popular technique. While there are many variations of this technique, suture material used, and types of securing implants, the consistent goal is to “mimic” the function of the ruptured CrCL with a suture placed in similar orientation to the original ligament. The long-term goal is to facilitate the formation of organized scar tissue periarticular (around the joint) that will provide stability even as the suture gradually stretches or breaks. The most common complications after this procedure involve failure of the suture and progressive development of arthritis. The main risk factors for complications with suture-based techniques are patient size and age; larger and younger patients have more complications. For these reasons, many surgeons reserve suture techniques for small breed, older, and/or inactive dogs. The main advantages of this technique include its typically lower cost, lack of required specialized training to perform, and the lack of a bone cut.
 The Tightrope® is a novel “suture” technique that was developed as an alternative to osteotomy-based techniques. It utilizes a specifically developed suture/toggle implant that requires holes to be drilled through the thigh (femur) and shin (tibia) bones for more accurate anatomic placement of the implant (Figure 5).Advantages of this procedure over other suture-based techniques include more accurate placement of the implant and better “suture” strength. A study comparing TPLO and Tightrope® techniques did not find a significant difference between them relative to outcomes at 6-months after surgery.
The Tightrope® is a novel “suture” technique that was developed as an alternative to osteotomy-based techniques. It utilizes a specifically developed suture/toggle implant that requires holes to be drilled through the thigh (femur) and shin (tibia) bones for more accurate anatomic placement of the implant (Figure 5).Advantages of this procedure over other suture-based techniques include more accurate placement of the implant and better “suture” strength. A study comparing TPLO and Tightrope® techniques did not find a significant difference between them relative to outcomes at 6-months after surgery.
Non-surgical treatment usually involves a combination of pain medications, exercise modification, joint supplements, physical rehabilitation, and possibly braces/orthotics.
- Activity restriction and anti-inflammatories – While administration of pain medications to dogs with CrCLD may improve their comfort, knee pain remains because of the persistent knee instability present. For this reason, strict activity restrictions (e.g., leash-based activities) are typically most effective at reducing pain in dogs with CrCLD. For these reasons, this treatment is generally limited to individual dogs in which surgery cannot be performed (i.e., financial constraints, illness, etc.)
- Rehabilitation therapy – There is ample evidence that therapy under the care of a veterinarian fully trained in physical rehabilitation can hasten and even improve the recovery from surgery. However, there is scant evidence to suggest that this is a consistent and predictable alternative to surgical management of CrCLD in dogs.
- Custom knee bracing/orthotics – Custom knee bracing is relatively new to canine orthopedics and there is no published data that supports it viability as a reasonable treatment in dogs with CrCLD. Much of the enthusiasm for dog knee bracing is extrapolated from their successful use in humans with ACL injuries. However, the mechanics of the canine and human knee are vastly different and it is unwise to make any comparisons between them relative to treatment modalities. At this time, there is not enough evidence to support any recommendation for knee bracing as a treatment of CrCLD.
Postoperative care at home is critical. Premature, uncontrolled or excessive activities risk complete or partial failure of any surgical repair. Such failure may require extensive surgery to address. Proper postoperative care will be explained to you in detail by your dog’s surgeon before and after surgery.
Studies show that physical rehabilitation can speed a dog’s recovery and improve final outcomes regardless of the chosen surgical technique. This rehabilitation should start immediately after surgery and usually includes a regime of passive range of motion, balance exercises, controlled walks on leash and so forth. Additional details should be discussed with a board-certified surgeon and/or a primary care veterinarian.
The long-term prognosis for animals undergoing surgical repair of CCLD is good, with reports of significant improvement in 85-90% of the cases. While, arthritis can progress regardless of treatment type, it’s expected to be slower when surgery is performed. Therefore, multimodal osteoarthritis management is recommended for any dog with CrCLD regardless of treatment. What this management might entail should be discussed with your dog’s surgeon and/or primary care veterinarian.
Obesity in pets has numerous health issues associated with it that go beyond CrCLD. Weight loss should be considered critical to any overweight pet with CrCLD. Your veterinarian can help you to determine the ideal weight of your pet and how best to reach it.


Tampa, FL 33615 (View map)
Tampa, FL 33647 (View map)
Tampa, FL 33617 (View map)


Tampa, FL 33647 (View map)